

EAE Induction by Active Immunization in SJL Mice
Recommended protocol for use with:
- Hooke Kit™ [Ser140]-PLP139-151/CFA Emulsion (cat. no. EK-0120)1,
- Hooke Kit™ [Ser140]-PLP139-151/CFA Emulsion PTX (cat. no. EK-2120), or,
- Hooke Kit™ PLP139-151 (native)/CFA Emulsion (cat. no. EK-0230)
1 EK-0120 was called "PLP139-151/CFA Emulsion" prior to May 2020. Only the name has changed, to avoid confusion with EK-0230.
Note: For kit EK-2120, this protocol version is for use only with Hooke PTX lot number 1012. (Other lots may require a different PTX dose.)
In this protocol "PLP139-151", without further qualification, refers to either [Ser140]-PLP139-151 or native mouse PLP139-151 peptide, as chosen by the investigator.
Contents
- Summary
- Kit selection
- Mouse selection
- Materials needed (per kit)
- Method
- Expected results
- Troubleshooting
- References
- Appendix A – Mouse EAE scoring guide
- Appendix B – EAE development in SJL mice
Summary
These kits are recommended for study of relapsing-remitting experimental autoimmune encephalomyelitis (EAE), including testing efficacy of potential therapeutics.
Each kit consists of:
- 3 pre-filled syringes with antigen in an emulsion with complete Freund's adjuvant, and,
- 1 vial of pertussis toxin in glycerol buffer (EK-2120 only)
EAE is induced in SJL mice by immunization with an emulsion of PLP139-151 in complete Freund's adjuvant (CFA). When using EK-2120, the initial immunization is followed by administration of pertussis toxin (PTX) in PBS on the day of immunization.
Most mice develop relapsing-remitting EAE with disease onset 9 to 14 days after immunization including PTX (EK-2120), or 10 to 15 days after immunization without PTX (EK-0120 or EK-0230). Peak of disease generally occurs 1 to 2 days after disease onset for each mouse, and lasts 1 to 3 days. Most mice completely or partially recover within 10 days. Usually 50 to 80% of mice will show an increase in EAE severity (relapse) after initial partial or complete recovery 20 to 40 days after immunization.
For study of only the first wave of EAE, we recommend 10 to 12 mice/group.
For study of EAE relapses, we recommend 15 to 20 mice/group. This relatively large number of mice is recommended to ensure that enough mice will relapse for good statistical analysis.
Mice are typically observed for 40 to 45 days after immunization. This is sufficient for at least 50% of mice to relapse.
Kit selection
EK-0120 and EK-2120 contain [Ser140]-PLP139-151 antigen.
EK-0230 contains native mouse PLP139-151 antigen ([Cys140]-PLP139-151), which induces more severe EAE.
EK-2120 is supplied with pertussis toxin (PTX); EK-0120 and EK-0230 are not. PTX induces a more severe initial wave of EAE, but it can also reduce the incidence of relapses.
Most labs will find kit EK-0120 suitable for study of either the initial wave of EAE, or for study of EAE relapses.
The table below summarizes the differences between the kits.
EAE induction kits compared (typical results)
| EK-0120 | EK-2120 | EK-0230 | |
|---|---|---|---|
| Antigen | [Ser140]-PLP139-151 | [Ser140]-PLP139-151 | Native mouse PLP139-151 |
| PTX | No | Yes | No |
| EAE onset1 | 11 to 15 days | 9 to 14 days | 10 to 14 days |
| EAE incidence | 90 to 100% | 90 to 100% | 90 to 100% |
| 1st wave severity | + | ++ | +++ |
| Relapse incidence | 50 to 80% | 20 to 50% | 50 to 80% |
1 Days from immunization
PLP139-151 induced EAE in SJL mice is sensitive to small variations in mice and in laboratory environments. (All testing at Hooke is with SJL mice from The Jackson Laboratory, stock #686).
If EAE severity with EK-0120 is insufficient, and the goal is to study the initial wave of EAE, we recommend kit EK-2120. The PTX in EK-2120 induces a more severe initial wave of EAE, but it can also reduce the incidence and severity of relapses.
If EAE severity with EK-0120 is insufficient, and the goal is to study EAE relapses, we recommend EK-0230, which uses the native mouse PLP peptide. This will induce more severe EAE than EK-0120, and will not reduce relapse incidence.
Mouse selection
For the most uniform EAE development, use female SJL/J mice at 8 to 9 weeks of age. All mice should be the same age.
Exclude any mice with tail lesions before immunization (see "Troubleshooting" below).
Hooke recommends and uses SJL mice from The Jackson Laboratory, stock #686.
Materials needed (per kit)
| Qty | Description |
|---|---|
| 1 | Hooke Kit™ [Ser140]-PLP139-151/CFA Emulsion (EK-0120) or Hooke Kit™ [Ser140]-PLP139-151/CFA Emulsion PTX (EK-2120) or Hooke Kit™ PLP139-151 (native)/CFA Emulsion (EK-0230) See "Kit selection" above. |
| 1 | 50 mL sterile polypropylene tube (EK-2120 only) |
| 10 | SJL mice, females, at 8 to 9 weeks old (The Jackson Laboratory strain SJL/J, stock #686) |
| Phosphate buffered saline (PBS; EK-2120 only) (standard formulation, pH 7.4, calcium-free, magnesium-free) |
Method
Overview
Acclimate mice for at least 2 weeks prior to immunization.
Administer each mouse adjuvant emulsion s.c. at 4 sites.
The same day, only if using Hooke Kit™ [Ser140]-PLP139-151/CFA Emulsion PTX (EK-2120), administer PTX in PBS, i.p.
Minimize mouse stress at all times (stress inhibits EAE development). See "Troubleshooting", below.
Preparation of pertussis toxin solution (for EK-2120 only)
Each EK-2120 kit comes with a vial containing 4 µg of PTX in 20 µg glycerol buffer (200 ng/µL). This PTX must be diluted with cold PBS (2 to 8 °C) for dosing.
For Hooke PTX lot 1012 we recommend the following PTX dosages:
- 30 ng PTX - to induce EAE while offsetting stress from dosing, or,
- 110 ng PTX - to induce EAE while increasing severity of the first wave of disease (this may decrease relapse)
These doses are the result of Hooke’s in vivo testing of the PTX lot (potency for EAE induction can differ up to 10 fold between PTX lots). Future lots may require different PTX doses.
Prepare PTX solution fresh (within 30 minutes before injection) under sterile conditions in a biosafety cabinet. Administer PTX after immunization with the emulsion component of the kit, the same day.
Important: The same solution of PTX must be administered to all mice. If more than one kit will be used in a study, prepare PTX for the entire study in one pooled batch.
To prepare the PTX solution:
Calculate the required volume of stock PTX in glycerol from the EK-2120 kit(s). Use the formula:
Number of mice * (PTX dose (ng) * 1.2) / 200 = µL
Example: 30 mice * (30 ng * 1.2) / 200 ng/µL = 5.4 µL
(This includes 20% extra PTX to allow for dosing loss.)
Put 0.12 mL cold PBS for each mouse into a single 50 mL sterile polypropylene tube. (The 0.12 mL includes 20% extra PBS to allow for dosing loss.)
Example: 30 mice * 0.12 mL = 3.6 mL PBS into the tube.
Note: This recommended dose is for Hooke PTX lot 1012 only; future lots may require different PTX doses.
Add PTX to PBS in 50 mL tube:
- Briefly centrifuge each PTX vial to ensure the liquid is at the bottom.
- Take the calculated volume of PTX stock (step 1 above) from the supplied vial(s), and place into the tube with PBS.
- Mix gently (do not vortex).
- Keep PTX solution on ice until injected. Inject all mice within 2 hours of preparation.
EAE induction



Good subcutaneous injection technique is important for successful EAE induction; the same person should inject all groups.
These procedures are drafted for right-handed injection; reverse if injecting with the left hand.
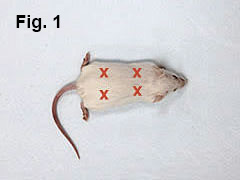
Anesthetize mouse per local IACUC and veterinary recommendations. Anesthesia is not required but Hooke recommends isoflurane anesthesia for efficient and precise immunization (figures here show anesthetized mice); for tips on restraining non-anesthetized mice, see our EAE induction protocol for C57BL/6 mice. (That reference is for mouse handling only; immunize SJL mice at 4 sites per this protocol.)
Lay mouse in prone position (belly down). Mouse will be immunized at 4 sites (Fig. 1).
Prime the needle by pushing a small amount of emulsion out onto a sterile tissue and wiping it off (Fig. 2).
With left hand, pinch skin over left shoulder. Using right hand, inject 0.05 mL of emulsion subcutaneously at that site (Fig. 3). Repeat the procedure by injecting 0.05 mL over mouse’s right shoulder.
Using a similar technique, inject 0.05 mL of emulsion over mouse’s left and right hip (Fig. 4).
After each injection, keep the needle inserted into the subcutaneous space for 10 to 15 seconds to avoid leakage of the emulsion. Alternatively, a light pull on the syringe plunger will prevent leakage.
Repeat steps 1 to 5 for all mice.
Perform steps 6 to 8 only if using Hooke Kit™ [Ser140]-PLP139-151/CFA Emulsion PTX (EK-2120):
Draw 1 mL PTX solution into 1 mL syringe.
Mount a fresh 27G ½" (12 mm) needle.
Inject each mouse i.p. with 0.1 mL.
Repeat steps 6 to 8 for all mice.
Check mice for signs of EAE daily starting 8 days after immunization. (See Appendix A below.)
Check mice for tail lesions regularly; exclude mice with tail lesions (see “Troubleshooting” below).
As soon as the first signs of paralysis occur, provide mice with food pellets and wet food on the floor of the cage, and HydroGel (ClearH2O, Portland ME) as a source of water. If mice are severely paralyzed (score 3 or greater), inject 1 mL Ringer’s solution s.c., daily or every other day.
All mice will develop obvious bumps of emulsion at the injection sites 2 to 4 days after injection.
In some mice, alopecia will develop at the site of injection 5 to 7 days after injection.
In most mice, the emulsion will remain at the site of injection for the duration of the experiment (typically 40 to 45 days). Approximately 10% of mice will clear the emulsion by developing small skin ulcers at injection sites. Most of the time, these ulcers do not require treatment – they usually heal in a few days and scars form. If concerned, consult attending veterinarian. Antibiotic ointment may be applied.
EAE development does not correlate with mice clearing or not clearing emulsion from the injection site.
Expected results
EAE will be consistently induced in 90 to 100% of mice, with disease onset in most mice occurring 9 to 14 days after immunization including PTX (EK-2120), or 10 to 15 days after immunization without PTX (EK-0120 or EK-0230). The mean maximum score of the first paralytic episode will be between 2.0 and 3.5 (the native PLP139-151 in kit EK-0230 will produce scores toward the higher end of the range).
Even mice that develop a very severe first wave EAE (score 4) will almost always show some recovery within 2 or 3 days; therefore euthanasia due to severe EAE is not needed in most cases. If mice are unable to reach water due to temporary paralysis, Ringer’s solution should be administered subcutaneously until recovery.
Mean maximum score of the second paralytic episode will be 1.5 to 3.5.
Daily dosing of mice often delays and reduces relapses due to stress of dosing.
The following illustrates typical results (results with undosed mice shown; vehicle-dosed mice will likely develop somewhat less severe EAE and will have lower incidence of relapses due to dosing stress):
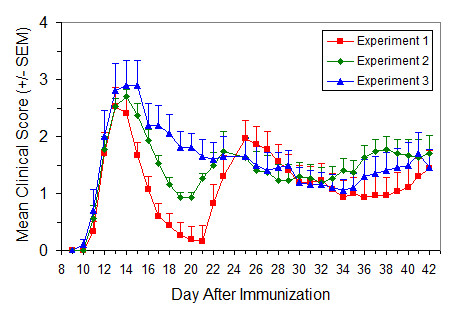
EAE induction in SJL mice
Protocol: EAE Induction by Active Immunization in SJL Mice
Data are from three independent experiments. Immunization used Hooke Kit™ [Ser140]-PLP139-151/CFA Emulsion (EK-0120), with female SJL mice.
| Exp. | # mice | Mean day of onset ± SD | MMS of 1st wave ± SD |
% EAE relapse | MMS of relapse1 ± SD |
MMS of relapse period (Days 21-42)2 ± SD |
End score (Day 42) ± SD |
Disease incidence |
|---|---|---|---|---|---|---|---|---|
| 1 | 15 | 13.3 ± 5.6 | 3.2 ± 0.5 | 87.0 % | 2.8 ± 0.6 | 2.7 ± 0.9 | 1.7 ± 1.2 | 100 % |
| 2 | 15 | 11.9 ± 0.6 | 2.7 ± 0.3 | 80.0 % | 2.9 ± 0.6 | 2.3 ± 1.3 | 1.4 ± 1.3 | 100 % |
| 3 | 10 | 12.3 ± 1.7 | 3.3 ± 0.9 | 80.0 % | 2.7 ± 0.7 | 2.7 ± 0.9 | 1.5 ± 1.0 | 100 % |
1 Only for mice which relapsed
2 For all mice in the group
Troubleshooting
In our experience, up to 10% of SJL mice may develop tail lesions for unclear reasons, either before or after immunization (development appears to be unrelated to immunization). Tail lesions appear as an area of raw skin, usually close to the root of the tail.
These may be mild (appears similar to a friction burn) to severe (appearance like a deep wound). If tail lesions develop after enrollment, apply antibiotic ointment immediately. If caught early (when lesions are mild), development of lesions can be reversed.
Mice with severe tail lesions will not develop EAE and should be excluded.
Successful induction of EAE requires low-stress mouse handling and husbandry procedures, good injection technique (as recommended above), use of appropriate mice, and good quality, stable, antigen emulsion.
Stress strongly decreases EAE susceptibility; minimizing mouse stress is very important for successful EAE induction.
For consistent EAE:
- Acclimate mice to your lab at least 2 weeks before starting.
- Follow recommended injection procedure. (See “EAE induction procedure” above).
- Check for tail lesions (see “Mouse selection and handling” above).
- Avoid excessive noise or vibration.
- Avoid excessive handling of mice. Handle mice gently.
- Try to do all procedures in the mouse room. Avoid moving mice on carts.
Isoflurane anesthesia may be used, and disease often develops better if mice are anesthetized during immunization.
References
[1] Lyons JA et al, Eur J Immunol 29:3432 (1999)
[2] Mendel I et al, Eur J Immunol 25:1951 (1995)
[3] Thornton V et al, Contemp Top Lab Anim Sci 42:49 (2003)
[4] Marusic S et al, J Exp Med 202:841 (2005)
[5] Thakker P et al, J Immunol 178:2589 (2007)
Appendix A - Mouse EAE Scoring Guide
Typically, EAE is scored on scale 0 to 5. Most researchers also give mice "in-between" scores (i.e. 0.5, 1.5, 2.5, 3.5) when the clinical picture lies between two defined scores.
The scoring method differs slightly depending on the stage of disease (onset/peak vs. recovery), for each individual mouse.
Reliable EAE scoring requires skill which comes after considerable experience. To avoid unconscious bias in scoring, we strongly recommend that mice should be scored blind, by a person unaware of which mice have received which treatment.
We recommend the following scoring guidelines for mice during onset and peak of EAE:
Mouse EAE scoring – onset and peak
| Score | Clinical observations |
|---|---|
| 0.0 | No obvious changes in motor function compared to non-immunized mice. When picked up by base of tail, the tail has tension and is erect. Hind legs are usually spread apart. When the mouse is walking, there is no gait or head tilting. |
| 0.5 | Tip of tail is limp. When picked up by base of tail, the tail has tension except for the tip. Muscle straining is felt in the tail, while the tail continues to move. |
| 1.0 | Limp tail. When picked up by base of tail, instead of being erect, the whole tail drapes over finger. Hind legs are usually spread apart. No signs of tail movement are observed. |
| 1.5 | Limp tail and hind leg inhibition. When picked up by base of tail, the whole tail drapes over finger. When the mouse is dropped on a wire rack, at least one hind leg falls through consistently. Walking is very slightly wobbly. |
| 2.0 | Limp tail and weakness of hind legs. When picked up by base of tail, the legs are not spread apart, but held closer together. When the mouse is observed walking, it has a clearly apparent wobbly walk. One foot may have toes dragging, but the other leg has no apparent inhibitions of movement. - OR - Mouse appears to be at score 0.0, but there are obvious signs of head tilting when the walk is observed. The balance is poor. |
| 2.5 | Limp tail and dragging of hind legs. Both hind legs have some movement, but both are dragging at the feet (mouse trips on hind feet). - OR - No movement in one leg/completely dragging one leg, but movement in the other leg. - OR - EAE severity appears mild when picked up (as score 0.0-1.5), but there is a strong head tilt that causes the mouse to occasionally fall over. |
| 3.0 | Limp tail and complete paralysis of hind legs (most common). - OR - Limp tail and almost complete paralysis of hind legs. One or both hind legs are able to paddle, but neither hind leg is able to move forward of the hind hip. - OR - Limp tail with paralysis of one front and one hind leg. - OR - ALL of:
|
| 3.5 | Limp tail and complete paralysis of hind legs. In addition to: Mouse is moving around the cage, but when placed on its side, is unable to right itself. Hind legs are together on one side of body. - OR - Mouse is moving around the cage, but the hind quarters are flat like a pancake, giving the appearance of a hump in the front quarters of the mouse. |
| 4.0 | Limp tail, complete hind leg and partial front leg paralysis. Mouse is minimally moving around the cage but appears alert and feeding. Often euthanasia is recommended after the mouse scores 4.0 for 2 days. However, with daily s.c. fluids most C57BL/6 mice may recover to 3.5 or 3.0, while SJL mice may fully recover even if they reach score 4.0 at the peak of disease. When the mouse is euthanized because of severe paralysis, a score of 5.0 is entered for that mouse for the rest of the experiment. |
| 4.5 | Complete hind and partial front leg paralysis, no movement around the cage. Mouse is not alert. Mouse has minimal movement in the front legs. The mouse barely responds to contact. Euthanasia is recommended. When the mouse is euthanized because of severe paralysis, a score of 5.0 is entered for that mouse for the rest of the experiment. |
| 5.0 | Mouse is spontaneously rolling in the cage (euthanasia is recommended). - OR - Mouse is found dead due to paralysis. - OR - Mouse is euthanized due to severe paralysis. |
In the recovery stage of EAE, most mice will have a tail that is no longer limp but is not normal either; it feels rigid and is "hooked". The hind legs may start moving (pedaling), but the mouse cannot walk. Either change makes scoring difficult.
We recommend the following modifications to the above scoring criteria for these mice:
Mouse EAE scoring – modified
| Score | Clinical observations |
|---|---|
| 0.0 | When held by the base of tail, tail is somewhat “hooked” and rigid, but tail makes complete rotations around the body axis (“helicopter”). Mouse is healthy. No signs of wobbling. |
| 0.5 | Mouse appears normal but tail is “hooked” and rigid. Tail does not make complete rotations around the body axis (“helicopter”). Mouse is healthy. No signs of wobbling. |
| 3.0 | Mouse is found on its side (as described for score 3.5 above), but there is excessive hind leg movement. Mouse cannot walk. - OR - Mouse has a wobbly walk (as described for score 2.5 above), and is unable to take more than two steps without falling on its side. The mouse is unable to right itself. - OR - Mouse has poor movement in the hind legs (as described for score 2.5 above), and has partial front leg paralysis evidenced by head held lower than normal and mouse's inability to right itself when placed on its side. |
| All other scores | Subtract 0.5 from the score of all mice with either a rigid, “hooked” tail or pedaling of hind legs. |
Relapses
Relapses are expected only in SJL mice, and only when EAE is induced by active immunization (vs. adoptive transfer).
Hooke's recommended criterion for EAE relapse is an increase in a score by one (1) full point from the lowest score of the remission.
For example, if an animal has an initial peak of disease with a maximum score at 3 and its score then drops to 0.5, the animal should then be considered to have relapsed on the day its score first reaches 1.5 or higher.
A small error in scoring can result in an incorrect detection of relapse. To help verify relapses, we recommend special attention to tail tension. Upon relapse, mouse tails will almost always become limp, similar to the limpness observed at EAE onset (see description of score 1.0). Observation of the newly limp tail is a confirmation of relapse.
For example, a mouse which has recovered to score 0.5 may have further scores of 0.5 or 1.0 without meeting the criterion for a relapse, but an additional increase of just one-half point (score 1.5 instead of 1.0) indicates a relapse. Even if the scoring technician is very experienced, it can be difficult to say if this increase represents a real relapse or a small scoring error. Observation of a clearly limp tail will help confirm that the recorded increase was a true relapse.
Appendix B – EAE Development in SJL Mice
Because of its many similarities to multiple sclerosis (MS), EAE is used to study pathogenesis of autoimmunity, CNS inflammation, demyelination, cell trafficking and tolerance induction.
EAE is mediated by myelin-specific CD4+ T cells, but CD8+ cells and B cells may also play a role in some models of EAE.
The relapsing-remitting EAE model in SJL mice is the mouse model which most closely resembles human MS.
The model is induced by immunization with [Ser140]-PLP139-151 in CFA emulsion, which may be followed by administration of pertussis toxin (PTX) in PBS if desired to increase severity of the first wave of EAE. The emulsion provides antigen which initiates expansion and differentiation of PLP-specific autoimmune T cells.
PTX enhances EAE development by providing additional adjuvant and facilitating entrance of autoimmune T cells into the CNS. However, in some labs PTX also reduces the incidence and severity of relapses in SJL mice.
This model is usually used to test efficacy of compounds on development of relapses in EAE. It is less often used in a prophylactic treatment study because most mice recover after the first wave of disease, even without treatment.
Most mice develop relapsing-remitting EAE with disease onset 9 to 14 days after immunization including PTX (EK-2120), or 10 to 15 days after immunization without PTX (EK-0120 or EK-0230). The first wave of EAE lasts several days and most mice fully or almost fully recover from it. After a disease-free period, which can last from one day to several months, most mice relapse.
Each individual mouse will have a different course of EAE after the first relapse. Most mice will only partially recover from the first relapse, but some may achieve full recovery. As mice are observed longer, more relapses will develop and less recovery will occur. During the first 5 to 7 weeks after immunization, 50 to 80% of mice will develop a relapse. After several months, almost all mice will have relapsed.
The first wave of paralysis occurs at the same time for all mice in the group, and is associated with a loss of body weight which is mostly regained on recovery from the first wave.
Different mice will experience succeeding waves of EAE at different times (not synchronized). In each wave there is body weight loss at onset (but not as dramatic as in the first wave), most of which is regained at recovery. After the first wave of disease, the average body weight of each group is relatively stable, with normal slow increases with age. This is because individual mice experience relapses at different times, so only a few mice in each group are acutely sick at any given time. Therefore, reliable differences in relative body weight (p < 0.05) between groups are not usually found at the end of the study (typically 40 to 45 days from immunization).
Both EAE incidence and severity will be reduced if mice are exposed to stress any time after approximately 3 days before immunization. Compound administration is a major source of stress; the more frequent the administration and the less tolerated the vehicle, the greater the reduction of EAE development. Unlike the therapeutic EAE model in C57BL/6 mice, in this model the stress of treatment and administration of vehicle continues to affect disease even after clinical signs of EAE appear.
The most important readouts in this model are incidence of relapse and MMS of the relapse period, calculated for all mice. The MMS of only those mice which relapse rarely shows meaningful differences between groups because only a fraction of mice relapse and relapse severity tends to be variable even within a single group. The MMS of the relapse period is more sensitive because it is based on all mice in the group and reflects both relapse severity and residual EAE severity in those mice which do not relapse.
Version: 2025-09-12
_150px.jpg)